
I’m getting scared.
I’m hearing a bunch of Republicans claiming that they are going to find ways to save money in Medicare. And, they are more naïve than I was in the early 1970s, when the goal was to convince Congress to pass HR1- the coverage of dialysis costs by the US Government. So the death panels (yes, they really existed) that made decisions as to who could be treated by dialysis and who would be left to die would no longer obtain.

Back then, there were only about 10,000 folks diagnosed with End Stage Renal Disease (ESRD). Who knew this would become VERY big business. With more than ¾ of a million folks covered by the Medicare program, which costs some $ 114 billion a year. (Note that the entire Medicare budget is all of $ 644 billion, which means almost 18 cents of every Medicare dollar is geared to the dialysis programs!)
I agree we have to find ways to save money. But, the logic (sic) these guys are spewing is very faulty.
Here are a few of their points.
- In 1973, 40% of the patients were treated at home. (Yes, that’s true. But, let’s not forget that the Kidney Center (National Medical Care’s name for its first dialysis clinic) was one of the few free-standing units at the time. Hospitals were providing acute dialysis or training patients to be treated at home. HR-1 was going to allow the number of clinics to explode- to some 5000 across the USA.)
- In 2020, 10% of patients undergo treatment at home. (That’s also true. But, that number also exceeds the total dialysis population that obtained about 5 years AFTER HR-1 was enacted.)
- HR-1 incentivized innovations that would benefit providers and preclude home care. (This is a bit of a stretch- almost as much as what Bob Gore effected with Teflon– that caused it to shatter into little pieces. If anything, it was the process by which HHS [Health and Human Services] reimbursed for dialysis- it disincentivized home dialysis- that created this situation.)
- In-Center treatment is expensive, exposes dialysis patients to various diseases (such a coronavirus right now), requires travel arrangements- and even more time relegated to a given treatment because of the transit time. By the way, the pandemic has increased the purchase of ACUTE (COVID-19 patients routinely suffer kidney failure) dialysis equipment by some 200%. (All of this is absolutely true.)
- Flattening the cost curve via price controls doesn’t’ work. (Really? Can you think of another medical program that has kept the price of a treatment virtually the same over 30+ years? Dialysis PER TREATMENT has remained virtually constant- it’s the NUMBER of patients that has elevated the overall costs.

- The smart play is to push dialysis back into the homes. (I certainly agree, but! Now, most dialysis patients are poorer than back in the 1970s. So, many live in small apartments. These domiciles may lack the space to perform dialysis. These folks are also going to need dialysis partners- trained folks who can help the patient institute dialysis and get them safely off the system when their treatment is finished. On the plus side, the patient can be treated every night- which will remove the spiky nature of their vitals that prevails with thrice weekly dialysis.)
- Starting next year (it was delayed one year), ESRD patients will be entitled to enroll in Medicare Advantage, which will help cover the costs that HHS doesn’t- like those directly related to home care. (Also true- as long as you read what I will discuss below.)
So, let’s consider what really is going to happen. The two big providers (Fresenius [the successor to National Medical Care, which was subsumed by Fresenius] and DaVita), plus many other providers will ride the pandemic to shift patients to home dialysis. This will let them sell more dialyzers (since re-use will be difficult for home patients to effect), as well as dialysis delivery systems. (Trust me- Fresenius notified its stockholders that this will be one of the profit drivers in the future. I’m not saying DaVita hasn’t made the same claim- I just haven’t been to their annual meeting or received their annual statement.)

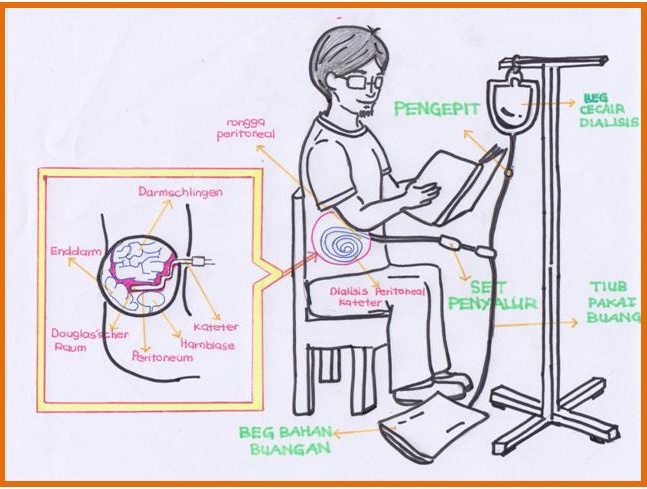
There also will be a concerted push to place hemodialysis patients into a peritoneal program. Many physicians consider peritoneal dialysis to be equivalent- it just needs to be effected more frequently (daily), involves more chance to complications, and some patients won’t (or can’t) accommodate it.
If hemodialysis is employed and not peritoneal dialysis
Dialyzer Reuse:
Right now, patients use one dialyzer (the ‘artificial kidney’) a month. For the past three decades, the cleansing and disinfection of dialyzers has been automated (quality control testing must be done after each reprocessing- that won’t happen at home), so the average dialyzer cost per treatment is about 1/10 the cost of using new dialyzers. This means the dialyzer costs for each treatment will be 10X as high. So, the cost savings for home treatment is going to take a big hit. The next “but” is the real killer.
Dialysis Delivery Machines:
Right now, clinics own (and maintain) one dialysis delivery machine for every 6 patients or so. That means the costs for these units (which are substantial) is spread over 6 patients. And, since the units are in a dialysis center, one technician is able to ‘maintain’ the units, clean them, etc. Once we move a patient to the home, it means ONE dialysis delivery unit will be used by ONE patient. That’s a substantial capital cost. (This is why Fresenius just dropped $ 2 billion to take over NxStage- it’s main product is a home dialysis delivery machine.) Plus, someone will have to visit the home at LEAST once a month (if not weekly) to ensure the unit is fully operational.
So, I see BETTER patient outcomes- with only very slight cost savings. (I fear Fresenius and DaVita see better patient outcomes with higher profits for their firms.)






This is something I don’t know, thanks you.
Steve Fan recently posted..Mitsume ga Tooru
Thanks for the visit and the compliment!
As a kidney transplant recipient (from a living donor), you are in my wheelhouse and speaking my language. I underwent both types of dialysis at different times but mostly peritoneal. I am a doctor so sterile technique was not a big issue for me. I do think that most patients could do peritoneal at home but aren’t offered the option. My nephrologist didn’t give me the option for hemo (she waved the “you’re a doctor” card at me) and I am so glad she did. I did undergo hemo for 3 weeks (after abdominal surgery) and it was so hard.
Our only hope is to prevent the kidney failure ( idealistic), make it easier to donate (benefits for living donors and an opt-out system for organ donation), and trying more folks on home dialysis. Peritoneal allowed me to at least attempt to have a regular life. Hemo took a day to recover from then it was time to go back,
Sorry for rambling on your post! It’s a bit personal for me!
Dominique Walton Brooks recently posted..Life Reset: Check Your Gut
I understand completely, Dominique! I’ve been involved with dialysis for more than 60 years- and think hemo is the way to go (we differ)- but with nocturnal, 5-7 X a week frequency. Glad your transplant’s been a success!
Medicare For All is the only answer. We did an economic Impact Study here in PA and an inconvenient truth, especially for Republicans, was revealed: we would save money, and everyone would be covered. What’s not to like?
Those folks who spent years (decades?) fighting for great union health benefits are the primary complainers. Not their employers, of course…
It seems like if this could be done at home it would make things easier for the patient but wow the expense. How can an average working person handle the expense without insurance?
Martha recently posted..Mini M&M’s
That is the problem for the first year of dialysis, Martha. Medicare used to pick up the tab after 9 months- now it’s doubled the waiting period.
My takeaway from this post is that they got the problems right, but were misguided or mistaken about the ideal solutions. And that they seem to be primarily motivated by profit.
I think your last sentence sums it up well, Jeanine.